![Medical News Asia | Powered by ['mediPr]](https://medi-paper.com/wp-content/uploads/2020/02/MediPR-MediPaper-Medical-Communications-Ltd-Healthcare-Writers-Medical-Writers-Medical-Writer-Agency-Hong-Kong-Medical-Writing-Services-Solutions-Quote-醫學寫作-香港-醫學作家香港-medical-PR-public-relations-1030x374.png)
By: Anaesthesiology.asia | Last updated: 24 December 2018 | In: Critical Care Medicine, Uncategorised
Article Keywords
Muscle relaxant, acetylcholine, NMBA, ACh, succinylcholine, aminosteroid, tracheal intubation, ARDS, atracurium, benzylisoquinoline, CCU, cisatracurium, ICU
During a recent webcast sponsored by Aspen and JS Vision Ltd held in Bangkok, Associate Professor Onuma Chaiwat discussed the role of neuromuscular blockade in improving outcomes in mechanically ventilated patients.
Associate Professor Onuma Chaiwat
Department of Anaesthesiology
Mahidol University, Thailand
Neuromuscular blocking agents (NMBAs) are commonly used in intensive care units (ICUs) as muscle relaxants, primarily to facilitate mechanical ventilation. They are divided into depolarising and non-depolarising NMDAs.1 The latter group, which is more often used in the ICU, is further classified into aminosteroid compounds and benzylisoquinoline compounds according to their chemical structure.1Appiah-Ankam J, Hunter JM. Cont Edu Anaesth Crit Care Pain 2004;4:1–7.
Non-depolarising NMBAs act as competitive antagonists to acetylcholine (ACh) at the postsynaptic nicotinic receptor.1Appiah-Ankam J, Hunter JM. Cont Edu Anaesth Crit Care Pain 2004;4:1–7. Binding of the agents to one or both α-subunits prevents ACh from depolarising the receptor, which eventually results in failure to produce muscle contraction.1Appiah-Ankam J, Hunter JM. Cont Edu Anaesth Crit Care Pain 2004;4:1–7.
Use of NMBA in critically ill patients
Benzylisoquinolines are widely used in the ICU for various indications, including the:2Greenberg SB, Vender J. Crit Care Med 2013;41:1332-1344.
i. Facilitation of tracheal intubation;
ii. Facilitation of mechanical ventilation and to aid oxygenation, for example in acute respiratory distress syndrome (ARDS);
iii. Facilitation of patient-ventilator synchrony for status asthmaticus;
iv. Control of persistently elevated intracranial pressure;
v. Reduction of abdominal wall muscle tone in patients with elevated intra-abdominal pressure;
vi. Prevention of shivering during therapeutic hypothermia;
vii. Reduction of muscle tone, for example in status epilepticus and tetanus;
viii. Facilitation of various other procedures and tests.
Non-depolarising NMBAs act as competitive antagonists to acetylcholine (ACh) at the postsynaptic nicotinic receptor.1Appiah-Ankam J, Hunter JM. Cont Edu Anaesth Crit Care Pain 2004;4:1–7. Binding of the agents to one or both α-subunits prevents ACh from depolarising the receptor, which eventually results in failure to produce muscle contraction.1Appiah-Ankam J, Hunter JM. Cont Edu Anaesth Crit Care Pain 2004;4:1–7.
The ideal properties of NMBAs for use in critically ill patients include the elimination independent of renal or hepatic function, no adverse cardiovascular (CV) effects, lack of metabolites with neuromuscular-blocking activity, absence of drug-drug interactions, and no accumulation over time, with a rapid and predictable on- and offset of effects.3Tripathi SS, Hunter JM. Cont Edu Anaesth Crit Care Pain 2006;6:119–23. The non-depolarising NMBAs, atracurium and cisatracurium are unaffected by renal and hepatic insufficiencies as the agents are metabolised mainly via Hofmann-degradation independent of organ function.1Appiah-Ankam J, Hunter JM. Cont Edu Anaesth Crit Care Pain 2004;4:1–7. These agents also do not produce any active metabolites with neuromuscular blocking activities, however, histamine-release associated with high dose atracurium is of concern. 1Appiah-Ankam J, Hunter JM. Cont Edu Anaesth Crit Care Pain 2004;4:1–7. Cisatracurium and vecuronium, on the other hand, do not release histamine, provide superior hemodynamic stability and have no important hemodynamic side effects.4Hemmerling TM, et al. Ann Card Anaesth 2008;11:80–90.
Attention should be given to factors which interfere with the action of NMBAs in critically ill patients. Advanced age reduces the rate of elimination of the agents, whereas hypothermia and electrolyte disturbances can prolong the effects of an NMBA.3Tripathi SS, Hunter JM. Cont Edu Anaesth Crit Care Pain 2006;6:119–23. Dysregulation of the ACh receptor is reported in several clinical conditions and affects the use of NMBAs. Upper and lower motoneuron lesions, muscle trauma, burn injury, immobilisation and sepsis all result in the upregulation of ACh receptors and subsequent decreased sensitivity to non-depolarising NMBAs leading to an increased requirement for the antagonists.5Martyn JA, et al. Anesthesiology 1992;76:822–43. Using the depolarising NMBA succinylcholine in these conditions is cautioned as it comes with a risk for hyperkalaemia.5Martyn JA, et al. Anesthesiology 1992;76:822–43. Conversely, conditions such as myasthenia gravis, organophosphorus poisoning and cholinesterase inhibition lead to the down-regulation of ACh receptors causing increased sensitivity to NMBAs.5Martyn JA, et al. Anesthesiology 1992;76:822–43. Finally, various drugs interact with NMBAs, resulting in either resistance to the agents or prolonged activity.3Tripathi SS, Hunter JM. Cont Edu Anaesth Crit Care Pain 2006;6:119–23.
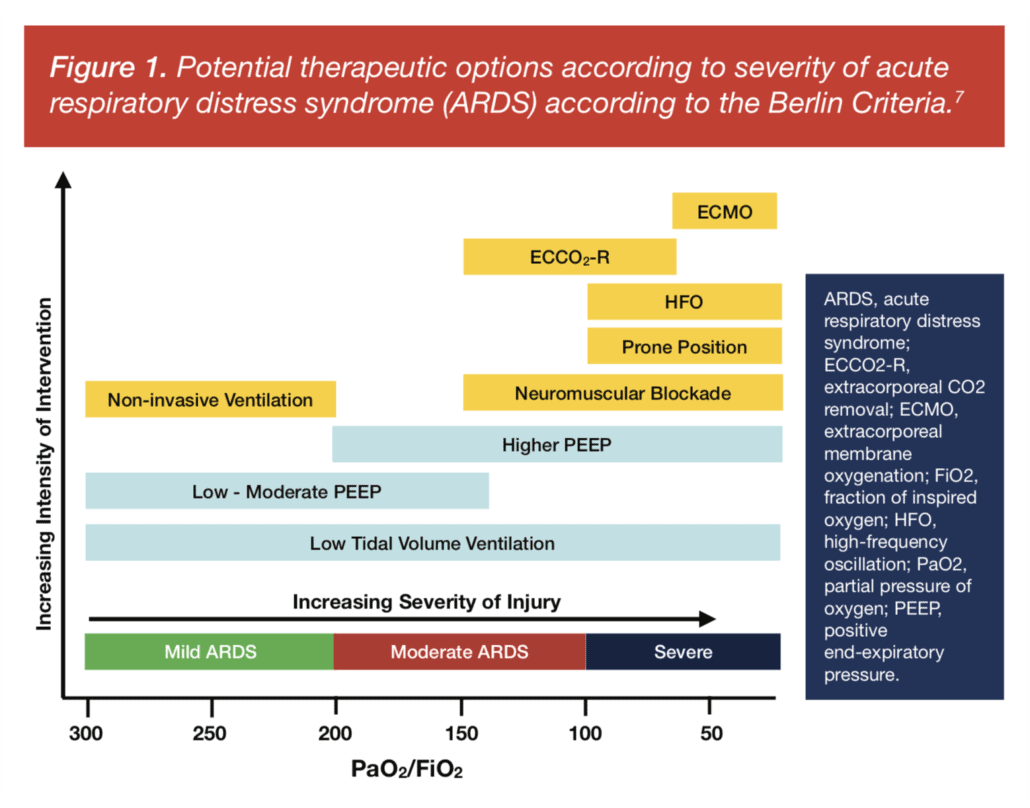
Figure 1. Potential therapeutic options according to severity of acute respiratory distress syndrome (ARDS) according to the Berlin Criteria.7Ferguson ND, et al. Intensive Care Med 2012;38:1573–82.
RECOMMENDED
NMBA in the treatment of ARDS
NMBAs are widely used to facilitate mechanical ventilation in patients with ARDS. Clinical practice guidelines suggest that neuromuscular blockade be administered by continuous intravenous infusion early in the course of ARDS for patients with a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <150.[mfn referencenumber=6]Murray MJ, et al. Crit Care Med 2016;44:2079–103.[/mfn] Figure 1 depicts therapeutic options for ARDS according to disease severity proposed by the European Society of Intensive Care Medicine, which recommends NMBA as a suitable therapy for Berlin-defined moderate-to-severe ARDS.7Ferguson ND, et al. Intensive Care Med 2012;38:1573–82.
In ARDS therapy, NMBAs enable the use of lung-protective ventilation strategies thus preventing ventilator-induced lung injury (VILI).8Yegneswaran B, Murugan R. Crit Care 2011;15:311.,9Cho YJ, et al. Tuberc Respir Dis (Seoul) 2016;79:214–33. The agent can be used to facilitate several therapeutic procedures in ARDS including prone positioning, permissive hypercapnia, extracorporeal membrane oxygenation with high positive end-expiratory pressure, and high-frequency oscillation ventilation.7Ferguson ND, et al. Intensive Care Med 2012;38:1573–82. NMBAs act via several mechanisms in these procedures including by increasing chest wall compliance, improving patient-ventilator synchrony, gas exchange, and systemic oxygenation, allowing for the accurate adjustment of tidal volume and pressure levels, reducing oxygen consumption by decreasing the work of breathing and respiratory blood flow, as well as decreasing lung or systemic infection.8Yegneswaran B, Murugan R. Crit Care 2011;15:311.,9Cho YJ, et al. Tuberc Respir Dis (Seoul) 2016;79:214–33.
NMBAs improve mortality in ARDS
Survival benefit is an important outcome from the use of NMBAs in ARDS. NMBAs reduce mortality in ARDS by eliminating active expiration following paralysis, thus decreasing VILI such as barotrauma, volutrauma and atelectrauma. This ultimately results in reduced release of inflammatory mediators and therefore prevents damage to vital organs and muscles.10Slutsky AS. N Engl J Med 2010;363:1176–80. Improved mortality with NMBAs in ARDS has been assessed in several studies. The largest trial to date, which studied 340 patients presenting to the ICU with an onset of severe ARDS within the previous 48 hours, showed that early administration of an NMBA improved survival at 90 days and increased time off a ventilator without increasing muscle weakness.11Papazian L, et al. N Engl J Med 2-1-;363:1107–16. It also decreased the incidence of barotrauma during the first 90 days.11Papazian L, et al. N Engl J Med 2-1-;363:1107–16. These findings were reiterated in a meta-analysis of three trials involving 431 patients from 20 centres.12Alhazzani W, et al. Crit Care 2013;17:R43. However, as studies on this subject are sparse, there remain several concerns and questions on the use of NMBA in ARDS, including whether the findings are applicable only to cisatracurium and optimal dosing strategies to adopt. This has led to the initiation of the ROSE study (Re-evaluation of Systemic Early Neuromuscular Blockade), a large randomised controlled trial that aims to confirm the beneficial effects of early NMBA administration on mortality in ARDS.13Huang DT, et al. Ann Am Thorac Soc 2017;14:124–33.
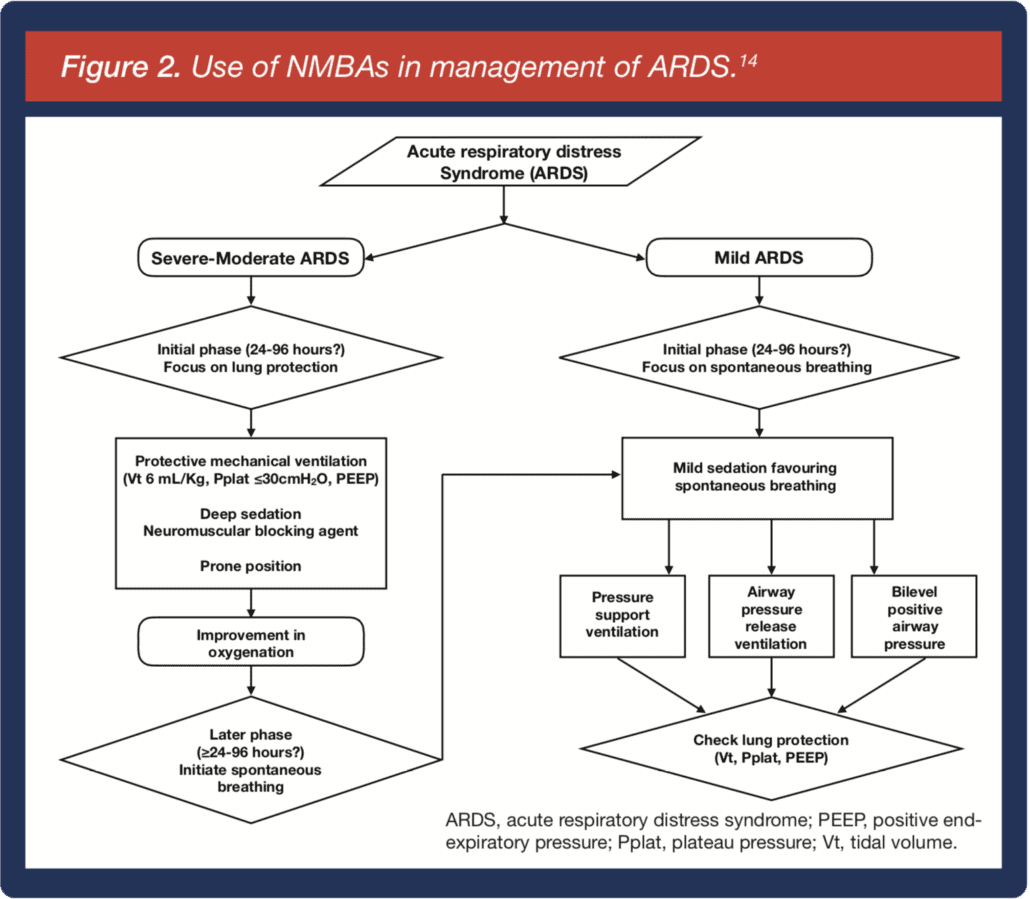
Figure 2. Use of NMBAs in management of ARDS.14Bourenne J, et al. Ann Transl Med 2017;5:291.
RECOMMENDED
Conclusion
NMBA can be used to improve outcomes in patients with ARDS, especially in moderate-to-severe disease. Figure 2 outlines the role of the agent in ARDS management.14Bourenne J, et al. Ann Transl Med 2017;5:291. Additionally, the following clinical pearls serve as important reminders when using NMBAs in the ICU to ensure best outcomes:
- Ensure the patient has received sufficient sedation prior to administering NMBAs.
- In patients with renal and/or hepatic insufficiency, atracurium or cisatracurium are preferred as they undergo Hoffman degradation and are less dependent on renal or hepatic function.
- In patients with CV disease, vecuronium may be preferred due to it having the least CV effects.
- Succinylcholine is the only available depolarising NMBA with rapid onset and brief duration of action and is mostly used for facilitating intubation. Hyperkalaemia is a potential side effect.
- Aminoglycoside antibiotics may enhance the effects of NMBAs.
Reference
- Appiah-Ankam J, Hunter JM. Cont Edu Anaesth Crit Care Pain 2004;4:1–7.
- Greenberg SB, Vender J. Crit Care Med 2013;41:1332-1344.
- Tripathi SS, Hunter JM. Cont Edu Anaesth Crit Care Pain 2006;6:119–23.
- Hemmerling TM, et al. Ann Card Anaesth 2008;11:80–90.
- Martyn JA, et al. Anesthesiology 1992;76:822–43.
- Murray MJ, et al. Crit Care Med 2016;44:2079–103.
- Ferguson ND, et al. Intensive Care Med 2012;38:1573–82.
- Yegneswaran B, Murugan R. Crit Care 2011;15:311.
- Cho YJ, et al. Tuberc Respir Dis (Seoul) 2016;79:214–33.
- Slutsky AS. N Engl J Med 2010;363:1176–80.
- Papazian L, et al. N Engl J Med 2-1-;363:1107–16.
- Alhazzani W, et al. Crit Care 2013;17:R43.
- Huang DT, et al. Ann Am Thorac Soc 2017;14:124–33.
- Bourenne J, et al. Ann Transl Med 2017;5:291.
Disclaimer
This article is not medical advice. Patients should seek personal assessment by a licenced specialist. Physicians are recommended to read the full publication(s) as cited in the article before making medical decisions. This article does not supersede nor replace the published article(s).
© Copyright 2018 Anaesthesiology.asia – Video: Prof Onuma Chaiwat on the ideal NMDA in ARDS patients
YOU MAY ALSO LIKE
© Copyright 2018 Anaesthesiology.asia – Video: Prof Onuma Chaiwat on the ideal NMDA in ARDS patients
Leave a Reply
Want to join the discussion?Feel free to contribute!